
Abstract
Purpose: The diagnosis of chronic pulmonary aspergillosis (CPA) is occasionally complicated due to poor sensitivity of mycological culture and colonization of Aspergillus species in the airway. Several diagnostic methods have been developed for the diagnosis of invasive pulmonary aspergillosis; however, their interpretation and significance are different in CPA.
This study aimed to review the recent advances in diagnostic methods and their characteristics in the diagnosis of CPA.
Recent findings: Radiological findings of lung, histopathology, and culture are the gold standard of CPA diagnosis. Serodiagnosis methods involving the use of galactomannan and β-D-glucan have low sensitivity and specificity.
An Aspergillus-specific IgG antibody assay showed good performance and had better sensitivity and reproducibility than conventional precipitant antibody assays. Currently, it is the most reliable method for diagnosing CPA caused by Aspergillus fumigatus, but evidence on its effectiveness in diagnosing CPA caused by non-fumigatus Aspergillus is lacking.
Newly developed lateral flow device Aspergillus and detection of volatile organic compounds in breath have potential, but evidence on its effectiveness in diagnosing CPA is lacking. Some of the azole-resistant-related genes can be detected directly from clinical samples using a commercially available kit. However, its clinical efficacy for routine use remains unclear.
Conclusion: Several issues surrounding the diagnosis of CPA remain unclear. Hence, further investigations and clinical studies are needed to improve the accuracy and efficiency of CPA diagnosis.
Introduction
CPA is a slowly progressive pulmonary disease caused by Aspergillus spp. and its prognosis is poor; the 5-year mortality rate of CPA patients is approximately 50–85%. CPA is categorized into five disease entities based on the recent guidelines of the European Respiratory Society: Aspergillus nodule, simple pulmonary aspergilloma, chronic cavitary pulmonary aspergillosis (CCPA), chronic fibrosing pulmonary aspergillosis (CFPA), and subacute invasive pulmonary aspergillosis (SAIA).
The diagnosis of CPA is occasionally complicated, as there are several disease entities in CPA, which are described in the following section, and some patients with underlying pulmonary diseases develop Aspergillus airway colonization.
Diagnostic methods used for CPA are similar with those of IPA, but their interpretation and significance are different. The present review describes the currently available diagnostic methods and discusses new approaches for diagnosing CPA and their future directions.
Radiological and histopathological findings
Simple pulmonary aspergilloma is defined as single pulmonary cavity containing a fungal ball in a non-immunocompromised patient with minor or no symptoms and no radiological progression over at least 3 months of observation.
On the contrary, CCPA and SAIA are characterized by one or more cavities with or without fungal ball and its radiological progression such as expanding thick-walled cavities and pericavitary infiltration. The crucial difference between them is that SAIA involves hyphal invasion into the lung parenchyma. CCPA usually occurs in pre-existing cavities, whereas in SAIA, cavities can be subsequently formed by the necrotic change of nodules or infiltration lesion due to Aspergillus species infection.
Thus, these three clinical entities are vague and overlapping in some cases; however, it is essential to distinguish them in order to estimate their prognoses. Although triazole antifungals are recommended in these entities, their efficacy was better in patients with SAIA than in those with CCPA.
Mycological culture
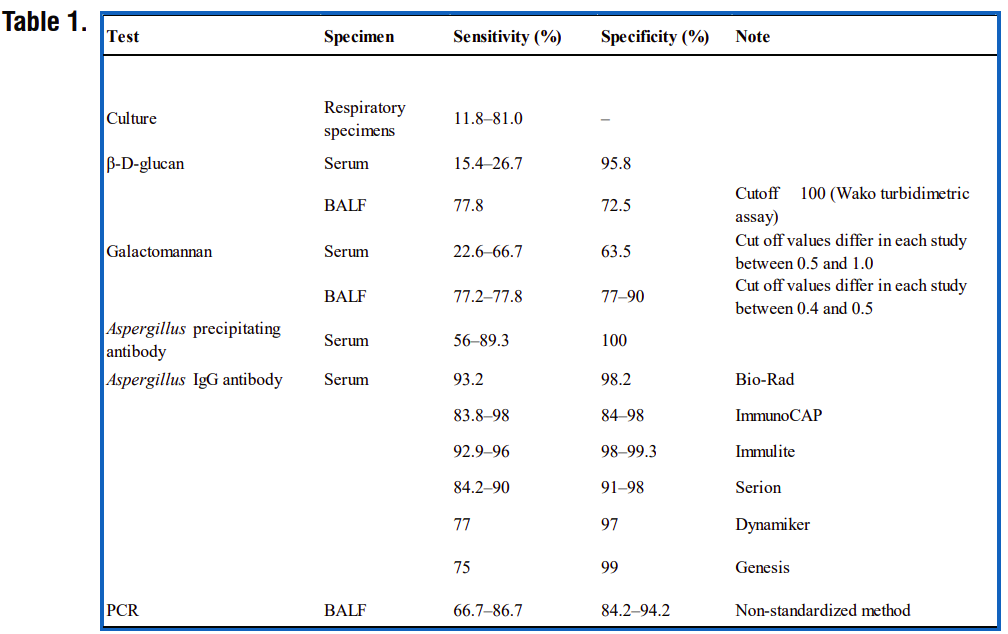
Mycological culture is the basic methods for diagnosing CPA, although it has several limitations. The culture positivity rates of Aspergillus species from respiratory specimens in CPA vary widely, ranging from 11.8 to 81.0% depending on reports. It was reported that 48 (63%) individuals were colonized patients among 76 non-granulocytopenic patients whose respiratory specimens yielded Aspergillus fumigates.
By contrast, 58 (65.9%) of 88 individuals were colonized patients whose cultures yielded non-fumigatus Aspergillus strains. These reports imply that the clinicians need to be careful when interpreting the results of fungal cultures from respiratory specimens. Therefore, we need a biomarker that reflects the invasiveness of Aspergillus infection.
Antigen and antibody test
Serodiagnosis is indispensable for the diagnosis of CPA. Galactomannan (GM) antigen assays in serum and bronchial alveolar lavage (BAL) fluid have high sensitivity and specificity for the diagnosis of IPA, with cutoff values of 0.5 and 1.0, respectively.
However, the GM serum assay has lower sensitivity and specificity for CPA, with a cutoff value of 0.5, than for IPA. GM antigen in BALF showed relatively higher sensitivity (77.2%) and specificity (77.0%), with a cutoff value of 0.4, than that in serum.
Recently, it was reported that the combination of GM and BDG assays in BALF had a higher diagnostic accuracy compared with other single or combinations of diagnostic methods including PCR.
Detection of the Aspergillus-specific antibody plays an important role in the diagnosis of CPA and Allergic bronchopulmonary aspergillosis and this method has been widely used. The precipitating Aspergillus IgG antibody has better sensitivity (80–90%) than GM and BDG assays.
Polymerase chain reaction (PCR)
Polymerase chain reaction (PCR) for the diagnosis of IPA has been used for over 2 decades. Aspergillus PCR from blood sample has similar sensitivity and specificity for the diagnosis of IPA but failed to detect Aspergillus DNA in patients with SPA and CPA, conversely, this implies that PCR could be useful to eliminate disseminated infection from CPA.
In BALF sample, PCR showed tolerable sensitivity (66.7–86.7%) and specificity (84.2–94.2%) compared to GM or BDG .
RT-PCR has advantages, (1) its quantitative aspect offers the possibility to establish precise cutoff values that could distinguish colonization from active infections, (2) since RT-PCR detects RNA, which is an indicator of the living fungal cells.
New strategies
Aspergillus-specific lateral flow device (LFD) was newly developed. It uses the mouse monoclonal antibody JF5, which binds to a protein epitope present on an extracellular glycoprotein antigen secreted constitutively during the active growth of A. fumigatus. This method can detect Aspergillus antigens in human serum within 15 min.
An early clinical trial showed that LFD is comparable to GM in serum in terms of diagnosing IPA, with a sensitivity and specificity of 81.8 and 98%, respectively. However, recently, a single center study reported that LFD showed low sensitivity of 38% for IPA. Volatile organic compounds (VOCs) are known to be detected from the breath of an infected individual. Initially, 2-pentylfuran was reported as the potential diagnostic VOC in IPA patients.
Galactosaminogalactan (GAG) is a newly discovered extracellular polysaccharide of Aspergillus species. It was observed only in hyphae form. GAG is particularly abundant in A. fumigatus. Furthermore, GAG is required for its virulence. Therefore, this component could be a potential biomarker to estimate the invasiveness of Aspergillus infection.
Diagnosis of infection
Azole antifungals are the mainstay of treatments for pulmonary aspergillosis. The mortality rates in IPA patients infected with azole-resistant strains were higher than those infected with azole-sensitive ones (88% vs. 30–50%).
The screening test with azole containing (itraconazole, 4 mg/L; voriconazole, 1 mg/L; posaconazole, 0.5 mg/L; and no antifungal) 4-well agar plate showed a sensitivity of 99% and a specificity of 99%, to screen the azole-resistant mutants; this could be useful and practical for routine test in clinical laboratories in countries where azole-resistance rate is high.
The most commonly used method is simple polymerase chain reaction (PCR) amplification of the entire coding and promoter region with sequence analysis of the PCR products; however, this method is not practical for clinical use as it is time consuming. Restriction fragment length polymorphism by AluI is valuable as it can detect TR34 and L89H mutations from DNA samples faster than sequencing.
In a multicenter clinical study, it showed good diagnostic performance on BAL and could detect A. fumigatus with resistance-associated mutations, including in culture-negative BALF samples, and detection of mutations was associated with azole treatment failure.
Diagnostic methods for CPA described in this review are summarized in Table1.
Conclusion
Needless to say, the gold standard of CPA diagnosis is the radiological findings of the lungs, its histopathology, and culture from the focus of infection. Other diagnostic tools are also dispensable and biomarkers to reflect the disease status are needed.
Currently, the Aspergillus-specific IgG antibody is the most promising tool for diagnosing CPA caused by A. fumigatus. We propose the algorithm for the diagnosis and treatment of CPA (Figure 1).
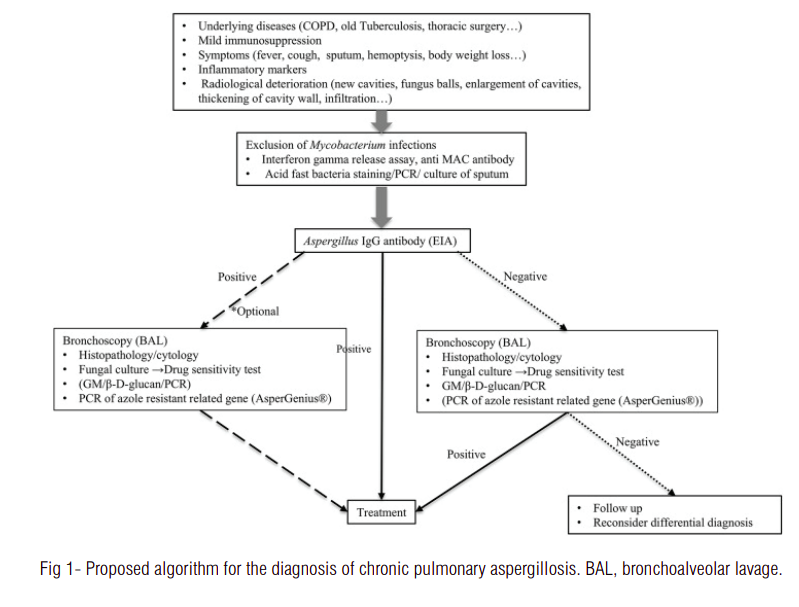
When the patient is suspected of chronic aspergillus infection, it is important to rule out the mycobacterium infection first. Indication of bronchoscopy examination should be considered depending on the result of Aspergillus IgG antibody test. If it is negative, bronchoscopy examination is strongly recommended, as non-fumigatus Aspergillus infection can be the causative organism. If it is positive, bronchoscopy examination is however, optional, to determine which antifungal agents to be used, or collect more precise epidemiological information.
Since the emergence of azole-resistant A. fumigatus strains is a serious concern, convenient detection methods are required to detect these directly from clinical samples; however, further investigation is required. In addition, we need to investigate how these azole mutants are produced inside the lungs and how they affect CPA patients to discover other methods to decrease their prevalence.
Source: Takazono, T., & Izumikawa, K. (2018). Recent Advances in Diagnosing Chronic Pulmonary Aspergillosis. Frontiers in microbiology, 9, 1810. https://doi.org/10.3389/fmicb.2018.01810


