
Introduction
(Article introduction authored by ICU Editorial Team)
In critically ill patients with acute respiratory failure, thoracic imaging plays a crucial role in evaluating disease nature, extent, and progression, guiding clinical management decisions. Computed tomography (CT) is the gold standard due to its detailed imaging capabilities, but limitations such as transportation and ionizing radiation exposure restrict its bedside use.
Chest X-ray and lung ultrasound (LUS) are increasingly viable alternatives, with LUS gaining prominence for its real-time applicability at the bedside. LUS facilitates dynamic assessments like “lung sliding” and supports prompt adjustments in mechanical ventilation and other therapies, potentially improving patient outcomes. Its popularity surged during the COVID-19 pandemic, enhancing its utility in intensive care settings.
Evolution of LUS in critically Ill patients
Since 1995, the American College of Radiologists has recommended daily supine chest X-rays for mechanically ventilated patients with acute cardiac and respiratory issues, regardless of the underlying condition.
Initially, these X-rays were crucial for identifying tube and central line malposition and detecting pneumothorax, leading to diagnostic or management changes in over 65% of cases.
The early 2000s marked significant advancements in critical care. The “Acute Distress Syndrome Network” in 2000 advocated for lung-protective ventilation strategies, reducing volotrauma incidence worldwide [6]. Concurrently, ultrasound-guided central venous catheter placement gained prominence, endorsed by healthcare agencies in the US and Europe, reducing iatrogenic pneumothorax rates.
Daniel Lichtenstein’s pioneering work between 1995 and 2009 introduced key ultrasound signs like “lung sliding” and the “lung point,” revolutionizing bedside ICU diagnostics and influencing therapeutic decisions [9-13]. His early studies demonstrated ultrasound’s immediate impact on patient management, paving the way for its widespread use in intensive care.
LUS and consolidation, interstitial syndrome, pneumothorax and pleural effusion
Daniel Lichtenstein pioneered comparisons of lung ultrasound (LUS) with auscultation and chest X-ray for diagnosing lung consolidation, showcasing LUS’s diagnostic superiority.
His “Bedside Lung Ultrasound in Emergency” (BLUE) protocol, featuring signs like the lung pulse and dynamic air bronchogram, advanced the role of LUS in diagnosing acute respiratory failure etiologies.
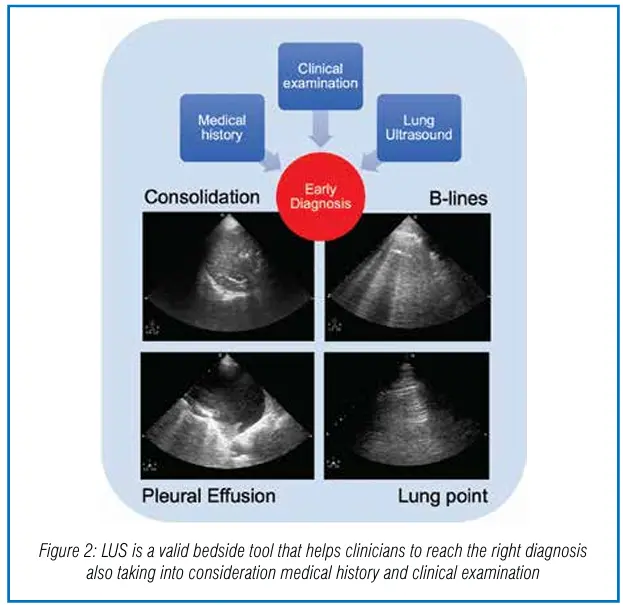
For instance, B-lines (formerly comet-tail artifacts) helped distinguish cardiogenic pulmonary edema from COPD exacerbation with high sensitivity and specificity. Pleural effusion (PE) is another example of the superiority of LUS compared to supine chest X-ray in ICU, where patients’ physical examination with percussion and auscultation have shown low sensitivity and specificity compared to CT scan as the
gold standard (Figure 2).
LUS has also excelled in pneumothorax (PNX) detection, outperforming chest X-ray with higher sensitivity (92%) and specificity (99.4%). In detecting pleural effusion (PE), LUS has shown superior accuracy compared to chest X-ray, crucially in ICU settings where physical exams and X-rays may lack sensitivity.

Estimating pleural effusion and improving accuracy in chest drainage positioning
Lung ultrasound (LUS) plays a crucial role in quantifying pleural effusion (PE) using various formulas, all showing good correlation with measured drainage volumes. The Balik formula, particularly popular for its simplicity, estimates PE volume by multiplying the maximal interpleural distance at the lung base by a constant factor.
However, it may overestimate volumes in specific conditions. In 2010, the British Thoracic Society (BTS) guidelines emphasized ultrasound-guided chest drain insertion for all pleural effusions to enhance safety and accuracy, following adverse events associated with blind procedures.
Recent ICU studies highlight that while pleural drainage significantly improves diagnostic accuracy and treatment decisions, it does not consistently impact outcomes like extubation success, weaning from non-invasive ventilation, or in-hospital mortality. Additionally, ultrasound’s utility in guiding chest drain insertion is limited in pneumothorax cases due to poor sound wave transmission through air.
LUS and fluid tolerance
Detecting fluid responsiveness and tolerance is crucial in managing critically ill patients, balancing between under-resuscitation and overhydration risks. Lung ultrasound (LUS) plays a pivotal role in assessing fluid tolerance by evaluating B-lines, which indicate interstitial syndrome with high accuracy compared to chest X-rays. For instance, B-profiles from base to apex suggest cardiogenic pulmonary edema, guiding against fluid administration. In ARDS, assessing B-lines helps distinguish interstitial syndrome from pulmonary edema, informing fluid management strategies that must balance oxygen delivery with avoiding exacerbating lung edema.
Advanced hemodynamic monitoring may be necessary, as B-lines correlate with extravascular lung water, influencing restrictive fluid strategies to improve outcomes like oxygenation. Conversely, the absence of B-profiles suggests “lung tolerance,” indicating fluid administration may be beneficial, particularly in shock scenarios.
Lung ultrasound score in ICU
Lung ultrasound (LUS) assesses lung aeration by scoring different patterns from 0 to 3: A-lines plus sliding, well-separated B-lines, coalescent B-lines, and consolidation. This score, first proposed by Soummer et al., aids in adjusting ventilation parameters, patient positioning, and predicting weaning outcomes. It has proven valuable in various clinical scenarios, such as predicting post-extubation
distress and evaluating lung reaeration in conditions like ventilator-associated pneumonia.
During the COVID-19 pandemic, LUS scores have been instrumental in predicting clinical deterioration and outcomes, correlating with survival rates and highlighting different disease sub-phenotypes. Notably, a new LUS-ARDS score has been proposed for non-COVID-19 ARDS patients, demonstrating comparable diagnostic accuracy to chest X-rays but with enhanced objectivity.
Lung ultrasound: basic and advanced skills
The use of ultrasound in ICU was categorized in 2009 by ACCP and SRLF, defining general critical care ultrasound (GCCU) for thoracic, abdominal, and vascular assessments, alongside critical care echocardiography (CCE) with basic and advanced levels.
Pleural ultrasound focused on guiding procedures and managing pleural fluid, while lung ultrasound (LUS) initially targeted pneumothorax detection post-procedure. The concept of monitoring lung aeration with LUS scores to evaluate ventilatory strategies was introduced in 2012.
Recent studies highlight challenges in skill differentiation between basic and advanced LUS, emphasizing the complexity of ruling in conditions like pneumothorax and consolidations. Mastering these skills requires extensive training due to their nuanced interpretation and variability in clinical settings.
Chest X-ray in ICU after 2012–2014
In 2006, Graat et al. demonstrated through routine chest X-rays in ICU that no new significant findings were identified in 2,457 exams on 754 patients. Subsequent studies and meta-analyses, including one by Oba and Zaza, found that eliminating daily routine chest X-rays did not affect ICU or hospital length of stay, ventilator days, or mortality rates.
Hendrikse et al. further supported this by analyzing 1,780 daily chest X-rays and finding diagnostic efficacy at only 4.4%. Consequently, the American College of Radiology updated their recommendations in 2011 and 2014, categorizing routine chest X-rays in stable ICU patients as “usually not appropriate”. Despite these guidelines, concerns and skepticism about the necessity of daily chest X-rays persist.
Chest X-ray vs LUS cost
Hejblum et al. compared daily chest radiographs versus a clinical-driven strategy in mechanically ventilated patients across 21 ICUs. They found a 32% reduction in chest X-rays with the clinical-driven approach, amounting to 35% fewer exams and a cost saving of $9,900 per bed per year, without compromising care quality or safety.
Scott et al. similarly demonstrated a 37% cost reduction in ICU monthly expenses by restricting daily chest X-rays, lowering costs from $11,633 to $7,348 post-intervention. Peris et al., after integrating LUS into their ICU practice, reported a 26% reduction in diagnostic chest X-rays and a 47% reduction in CT scans, resulting in a 39% reduction in radiological examination costs. Implementing LUS also led to a 57% decrease in chest X-ray costs, while CT scan rates remained unchanged, highlighting substantial cost savings without adverse effects on patient outcomes.
Limitations of chest X-ray vs LUS
Bedside portable chest X-rays have limitations in image quality and in accurately diagnosing critical causes of dyspnea such as pleural effusion, pneumothorax, pulmonary edema, and embolism. They can miss 10-25% of pleural effusions and 30% of pneumothoraxes. Chest X-rays are moderately specific (76%, 83%) but not sensitive enough (67-68%) for diagnosing heart failure, where echocardiography is crucial.
They also have low sensitivity for pulmonary embolism [83]. While LUS has many advantages, it has lower sensitivity compared to chest CT, exploring only 70% of the lung surface, which affects its ability to detect intraparenchymal pneumonia not adherent to the pleural surface. LUS can be challenging in obese patients and is hindered by subcutaneous emphysema.
Chest X-ray and irradiation
When considering radiological imaging techniques, it’s crucial to integrate appropriateness with radioprotection concerns. Exposure to ionizing radiation carries stochastic biological effects, where even low doses can potentially induce cancer or hereditary diseases, following a linear-no-threshold dose-response relationship.
While data on high-dose exposures are clearer, such as from atomic bomb survivors, uncertainties remain regarding low-dose exposures below 100 milliSievert (mSv). For instance, a single chest X-ray delivers about 0.02 mSv, while a chest CT is equivalent to 300-400 chest X-rays (6-8 mSv).
Therefore, minimizing radiation exposure, especially in repeated examinations and among vulnerable populations like children and women, aligns with the ALARA principle (as low as reasonably achievable).
Considering these risks, alternative imaging methods like LUS should be favored when feasible, provided they offer comparable diagnostic accuracy.
Further direction with LUS in ICU
Lung ultrasound (LUS) is now crucial in ICU settings, offering real-time imaging that integrates with clinical data to influence medical decisions swiftly.
It aids in adjusting ventilator settings, fluid management, patient positioning, antibiotic strategies, and chest drainage, enhancing patient care and potentially reducing reliance on chest X-rays, thus benefiting both economics and the environment.
Despite its operator-dependence and learning curve, ongoing research explores AI-driven algorithms for standardized LUS interpretation. Contrast-enhanced ultrasound (CEUS) shows promise in characterizing consolidations without the radiation exposure of CT scans. Experimental studies on LUS sliding velocity aim to refine ventilation strategies and PEEP titration in mechanically ventilated patients.
Conclusion
In this review, we’ve examined the evolution of lung ultrasound (LUS) and the decline of chest X-ray usage in ICUs over the past three decades, emphasizing pivotal advancements.
LUS has emerged as a critical tool for enhancing patient safety, enabling rapid bedside diagnosis, and facilitating ongoing patient monitoring.
We’ve also addressed economic considerations and the reduction of patient radiation exposure, advocating for minimizing routine supine chest X-rays in favor of integrating LUS into ICU practices.
Key challenges include the need for skilled operators, standardized image acquisition, and uniform reporting protocols. Looking ahead, advancements in technology may enable real-time bedside review of LUS images and continuous monitoring of patient progress in the ICU.


