Introduction
Nosocomial pneumonia, encompassing hospital-acquired pneumonia (HAP) and ventilator-associated pneumonia (VAP), is a major cause of mortality among critically ill patients. A growing number of cases are attributed to multi-drug-resistant Gram-negative bacteria (MDR-GNB), which complicates treatment due to the limited effectiveness of conventional antibiotics. These infections often lead to delayed therapy, prolonged hospital stays, and increased morbidity and mortality. The higher toxicity profiles of the antibiotics needed to combat MDR-GNB further exacerbate the challenges in managing such cases. The urgency to develop new antibiotics that can target these resistant pathogens is evident as existing treatments struggle to keep pace with evolving bacterial resistance.
In response, several novel antibiotics have been approved in recent years, offering hope for treating MDR-GNB nosocomial pneumonia. These include drugs like ceftolozane-tazobactam, ceftazidime-avibactam, and meropenem-vaborbactam, which demonstrate efficacy in both clinical and microbiological trials. Despite these advancements, the emergence of resistance to these new treatments underscores the need for judicious use to maintain their effectiveness.
The review also illustrates key physiological differences between normal alveoli and those affected by critical illness and pneumonia in Figure 1. This figure highlights the challenges antibiotics face in penetrating the infected lung tissue. For a drug to be effective in treating lung infections, it must reach the epithelial lining fluid (ELF) and achieve concentrations above the minimum inhibitory concentration (MIC). Figure 1 demonstrates how these critical illness-induced changes can impact drug delivery and efficacy, making it crucial to understand how altered physiology affects antibiotic performance, particularly in patients with severe infections.
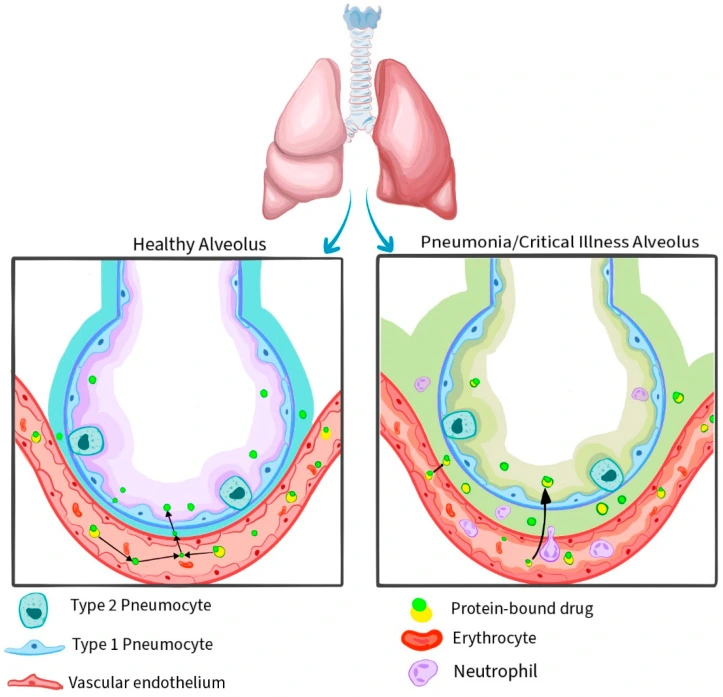
Figure 1: Physiological causes of differences in pharmacokinetic and pharmacodynamic parameters of antibiotics between normal alveoli and critical illness/pneumonia alveoli.
Ceftolozane–Tazobactam
In 2019, the FDA approved ceftolozane–tazobactam for treating hospital-acquired bacterial pneumonia (HABP) and ventilator-associated bacterial pneumonia (VABP) in adults. This combination of a fifth-generation antipseudomonal cephalosporin and a β-lactamase inhibitor targets some Ambler class A and C β-lactamases, including most ESBLs, but is ineffective against KPCs, OXA, and metallo-β-lactamases.
Both drugs are primarily excreted via the kidneys, requiring dose adjustments for renal impairment. In nosocomial pneumonia, a higher dose of 3 g every 8 hours is recommended, which is well tolerated. Clinical studies showed adequate lung penetration, achieving high target attainment in both plasma and the epithelial lining fluid (ELF), ensuring therapeutic levels throughout the dosing interval.
In Vitro Activity
Ceftolozane–tazobactam has strong antipseudomonal activity, making it the most effective β-lactam against Pseudomonas aeruginosa in several studies. It was found to inhibit 96% of P. aeruginosa isolates and 91.8% of Enterobacterales from lower respiratory tract infections (LRTIs), with 98% of Enterobacterales also susceptible to meropenem.
In pneumonia patients, ceftolozane–tazobactam inhibited 97.5% of P. aeruginosa isolates, including 87.9% of MDR and 82.9% of XDR strains, and 90.8% of meropenem-resistant isolates. It also showed >90% efficacy against Enterobacteriaceae, including 81.5% of ESBL-producing non-CRE strains.
Clinical Trials
The ASPECT-NP trial compared ceftolozane–tazobactam to meropenem in 726 patients with ventilated hospital-acquired pneumonia (HAP). Ceftolozane–tazobactam was found to be non-inferior to meropenem in terms of 28-day mortality and clinical cure rates. It showed effectiveness against Pseudomonas aeruginosa and ESBL-producing Enterobacterales, with lower mortality rates in the ceftolozane–tazobactam group. Microbiological eradication was similar for both treatments, and the double dose of ceftolozane–tazobactam was shown to be safe.
Real-world data from 33 studies reported clinical success rates from 51.4% to 100% in treating nosocomial pneumonia with ceftolozane–tazobactam, particularly against MDR/XDR P. aeruginosa. While it is a promising option for carbapenem-sparing therapy, resistance development, especially in P. aeruginosa, remains a concern. Overall, ceftolozane–tazobactam is valuable for treating pneumonia caused by MDR P. aeruginosa and ESBL-producing Enterobacterales, but further research is needed to solidify its role in guidelines.
Ceftazidime–Avibactam
In 2018, the FDA approved ceftazidime–avibactam for the treatment of hospital-acquired and ventilator-associated bacterial pneumonia. Avibactam, a non-beta-lactam β-lactamase inhibitor, restores ceftazidime’s activity against Ambler class A (e.g., ESBLs, KPCs), class C (e.g., AmpC), and some class D β-lactamases (e.g., OXA-48), but it is ineffective against class B metallo-β-lactamases. Phase 1 studies showed satisfactory lung penetration and no serious adverse effects, even at high doses. The dose is adjusted for renal function, and in vivo studies demonstrated a post-antibiotic effect against P. aeruginosa.
In Vitro Activity
In an in vitro study, ceftazidime–avibactam showed high susceptibility rates against respiratory pathogens: 97% for Enterobacter spp., 98.5% for Escherichia coli, 94.7% for Klebsiella pneumoniae, and 91.2% for Pseudomonas aeruginosa. It was effective against >88% of MDR pathogens but was less effective against MDR P. aeruginosa (65.7%) and XDR pathogens (<70%). Studies showed 91.7% of P. aeruginosa isolates and 84.7% of carbapenem-resistant strains were susceptible to ceftazidime–avibactam. In the REPROVE trial, 98.6% of Enterobacteriaceae and 88.4% of P. aeruginosa were susceptible to the drug.
Clinical Trials
The phase 3 REPROVE study assessed ceftazidime–avibactam (2 g ceftazidime plus 0.5 g avibactam) for nosocomial pneumonia versus meropenem. Ceftazidime–avibactam showed non-inferiority in clinical cure rates (68.8% vs. 73%), with similar all-cause mortality and microbiological eradication rates. Serious adverse events were rare (1%).
Further trials indicated a 55% clinical success rate in patients with carbapenem-resistant Enterobacteriaceae infections, but only 36% in those with pneumonia. Studies suggest ceftazidime–avibactam is superior to colistin for treating KPC-producing CREs. However, resistance emergence is a concern, linked to mutations in blaKPC and PDC genes, affecting susceptibility.
In conclusion, ceftazidime–avibactam is viable as first-line or salvage therapy for CRE-related pneumonia, emphasizing rapid CRE detection for timely treatment. Continuous infusion may enhance outcomes.
Meropenem–Vaborbactam
Meropenem–vaborbactam was approved by the EMA in 2018 for nosocomial pneumonia treatment. Vaborbactam, a cyclic boronic acid β-lactamase inhibitor, enhances meropenem’s activity against class A and C β-lactamases, including KPCs and ESBLs, but not against class B MBLs or OXA-48. Its effectiveness against P. aeruginosa and A. baumannii is limited, particularly when carbapenem resistance isn’t due to β-lactamase production.
The recommended dosage is 4 g (2 g meropenem and 2 g vaborbactam) every 8 hours as a 3-hour infusion, adjusted for renal function. Both drugs show good pulmonary penetration, with AUC ratios of 65% for meropenem and 79% for vaborbactam in healthy volunteers.
In Vitro Activity
An in vitro study of 4,790 Enterobacterales isolates from HAP/VAP patients in the US revealed that over 99.9% were susceptible to meropenem–vaborbactam, with 98.5% of CRE isolates also susceptible. However, resistance was observed in NDM-1 and IMP producers. For P. aeruginosa, meropenem–vaborbactam inhibited 89.5% of isolates, with lower rates for MDR (59.0%) and XDR (48.6%) strains.
In a European study, 98.0% of Enterobacterales were susceptible to meropenem–vaborbactam, inhibiting 99.1% of KPC producers but only 82.1% of P. aeruginosa strains. Notably, meropenem–vaborbactam was the least effective agent for P. aeruginosa compared to other β-lactam–β-lactamase inhibitors, with 88.7% susceptibility, while colistin showed the highest activity at 99.5%.
Clinical Trials
In the TANGO II trial, meropenem–vaborbactam was compared to best available therapy in 75 patients with suspected CRE infections, including 9.3% with HAP/VAP. In confirmed cases, meropenem–vaborbactam showed higher clinical cure (65.6% vs. 33.3%, p = 0.03) and microbiological eradication rates (65.6% vs. 40.0%, p = 0.09). It was linked to lower 28-day all-cause mortality and fewer adverse events, particularly nephrotoxicity. However, resistance was noted in five K. pneumoniae isolates.
Other studies indicated that meropenem–vaborbactam effectively treated KPC-producing K. pneumoniae infections, with a clinical success rate of 67% in patients with pneumonia. A comparison with ceftazidime–avibactam suggested that meropenem–vaborbactam might have lower rates of emergent resistance, but further studies are necessary.
Overall, meropenem–vaborbactam is a promising option for treating pneumonia caused by KPC-producing CRE Enterobacteriaceae, though rapid detection of KPC enzymes is crucial for timely treatment.
Imipenem–Cilastatin–Relebactam (Imipenem–Relebactam)
In 2020, the FDA approved imipenem–cilastatin–relebactam for treating HABP and VABP. Relebactam is a non-β-lactam diazabicyclooctane (DBO) inhibitor effective against Ambler class A (ESBLs, KPCs) and class C (AmpC) β-lactamases. It is also active against carbapenem-resistant P. aeruginosa but does not improve imipenem’s efficacy against OXA-48 carbapenemases or enhance its activity against certain inherently resistant species.
The approved dosage is 500/500/250 mg every 6 hours via a 30-minute intravenous infusion, with adjustments needed for renal insufficiency. Imipenem–relebactam shows good lung penetration, with satisfactory AUC ratios for both components.
In Vitro Activity
In a study of lower respiratory tract samples from Western Europe, 99.1% of Enterobacterales and 96.0% of piperacillin–tazobactam-resistant strains were susceptible to imipenem–relebactam. It inhibited 91.4% of P. aeruginosa, 73.5% of piperacillin–tazobactam-resistant strains, and 40.5% of meropenem-resistant strains. In Northern and Central Europe, it was effective against 99.6% of non-Morganellaceae Enterobacterales and 100% of ESBL-positive E. coli, K. pneumoniae, and K. oxytoca.
Imipenem–relebactam showed high activity against P. aeruginosa, with 97.3% susceptibility among respiratory isolates. It retained effectiveness against 50% of strains that became resistant to ceftolozane–tazobactam and 60.7% of those resistant to ceftazidime–avibactam. Notably, 58-59% of MDR P. aeruginosa resistant to ceftolozane–tazobactam remained susceptible to imipenem–relebactam, indicating different resistance mechanisms.
In a study from China, 84.2% of P. aeruginosa and 65.8% of MDR strains were susceptible, while only 22.2% of A. baumannii and 5.3% of MDR A. baumannii showed susceptibility to imipenem–relebactam.
Clinical Trials
The RESTORE-IMI 1 phase 3 trial compared imipenem–relebactam with imipenem–colistin for treating Gram-negative infections caused by imipenem-non-susceptible bacteria. Among 31 patients, 87.5% of those receiving imipenem–relebactam had a favorable outcome compared to 66.7% in the imipenem–colistin group, with lower 28-day mortality and nephrotoxicity in the former.
The RESTORE-IMI 2 trial evaluated imipenem–relebactam against piperacillin–tazobactam in patients with HAP/VAP. The 28-day mortality was 15.9% for imipenem–relebactam and 21.3% for piperacillin–tazobactam, showing non-inferiority. Favorable clinical response rates were 61.0% and 55.8%, respectively.
Resistance mechanisms for imipenem–relebactam include porin loss and increased blaKPC copy numbers. It is an effective treatment for difficult-to-treat P. aeruginosa and CRE infections, except for those producing MBLs or OXA-48-like carbapenemases. It may serve as rescue therapy for resistance to ceftolozane–tazobactam and ceftazidime–avibactam.
Cefiderocol
Cefiderocol was FDA-approved in 2020 for treating HABP/VABP. It is a novel siderophore cephalosporin effective against all four Ambler classes of β-lactamases, including ESBLs, KPCs, MBLs, and OXAs. It targets carbapenem-resistant P. aeruginosa, A. baumannii, and S. maltophilia, but not Gram-positive or anaerobic pathogens.
The recommended dose is 2 g infused over 3 hours every 8 hours, with adjustments for renal impairment. In healthy subjects, cefiderocol showed comparable lung penetration to other β-lactams, with a ratio of 10.1% in ELF to total plasma. In pneumonia patients, the lung penetration ratio reached 34%. Prolonged infusions are supported by in vivo studies in rat models against resistant bacteria.
In Vitro Activity
Cefiderocol is the most effective agent against carbapenem-resistant Enterobacterales (CRE), inhibiting 98.2% of isolates, outperforming meropenem–vaborbactam, imipenem–relebactam, and ceftazidime–avibactam. It also inhibited 95.1%, 95.9%, and 89.2% of isolates resistant to these agents, respectively. Susceptibility rates for P. aeruginosa and XDR isolates were 99% and 97.3%, while A. baumannii showed a 97.7% susceptibility rate. Resistance to cefiderocol was found in less than 1.5% of Enterobacterales, P. aeruginosa, A. baumannii, and S. maltophilia isolates.
Clinical Trials
The phase 3 APEKS-NP study showed that cefiderocol is non-inferior to meropenem for treating Gram-negative nosocomial pneumonia, with similar all-cause mortality rates at day 14 (12.4% for cefiderocol vs. 11.6% for meropenem). Common pathogens included K. pneumoniae, P. aeruginosa, and A. baumannii. Both drugs had a high ESBL-positive rate among Enterobacterales. The CREDIBLE-CR study compared cefiderocol with the best available therapy for carbapenem-resistant infections, showing a clinical cure rate of 50% for cefiderocol. However, it had a higher 14-day mortality (25% vs. 11%) largely due to A. baumannii. Overall, cefiderocol is effective against MDR Gram-negative infections, but further studies are needed to establish its role in salvage therapy, especially for CRAB infections.
Sulbactam–Durlobactam
In 2023, the FDA approved sulbactam–durlobactam for treating HABP and VABP caused by the Acinetobacter baumannii–calcoaceticus complex. This combination includes sulbactam, which has intrinsic activity against Acinetobacter spp., and durlobactam, a next-generation β-lactamase inhibitor that protects sulbactam from various β-lactamases. The recommended dose is 1 g/1 g infused over 3 hours every 6 hours.
In vitro studies demonstrate that sulbactam–durlobactam effectively inhibits 97.7% of A. baumannii isolates, with a MIC90 of 2 μg/mL for respiratory infections. Notably, only 46% of isolates were susceptible to meropenem, while 95.3% were susceptible to colistin. Resistance to sulbactam–durlobactam was low, with 2.3% of isolates showing resistance linked to MBLs or mutations in penicillin-binding protein-3 (PBP3). Additionally, in colistin-resistant A. baumannii isolates, 89% were susceptible to sulbactam–durlobactam, with increased susceptibility observed when combined with imipenem.
Clinical Trials
In the phase 3 ATTACK trial, sulbactam–durlobactam demonstrated non-inferiority to colistin for treating Acinetobacter baumannii–calcoaceticus complex infections, with both drugs administered alongside imipenem. Most patients had HAP, VAP, or ventilated pneumonia, and 69% of isolates were carbapenem-resistant. Day 28 all-cause mortality was 19% in the sulbactam–durlobactam group compared to 32% in the colistin group, which also had higher nephrotoxicity rates.
In conclusion, sulbactam–durlobactam offers a new treatment option for resistant Acinetobacter infections, but future studies need to validate its efficacy in real-world settings, clarify its use as monotherapy versus combination therapy, and assess its effectiveness against other types of ABC infections beyond HAP and VAP.
Conclusions
Antimicrobial resistance poses a growing challenge for clinicians, leading to delayed or inadequate treatment and poorer outcomes. In the past decade, new antibiotics targeting multidrug-resistant (MDR), extensively drug-resistant (XDR), and difficult-to-treat (DTR) Gram-negative bacteria have been approved, often with improved safety profiles compared to older options like colistin.
Key antibiotics include ceftazidime–avibactam, meropenem–vaborbactam, and imipenem–relebactam for carbapenem-resistant Enterobacterales (CRE), while options for DTR P. aeruginosa include ceftazidime–avibactam and ceftolozane–tazobactam. However, effective treatments for metallo-beta-lactamase (MBL) producers and carbapenem-resistant A. baumannii are limited. Cefiderocol exhibits broad-spectrum activity but is recommended for use in combination for A. baumannii. Sulbactam–durlobactam shows promise for CRAB pneumonia.
Comparative efficacy data for the new β-lactam–β-lactamase inhibitors and cefiderocol are lacking, necessitating further large-scale studies to determine the best treatment options for MDR Gram-negative bacterial pneumonia. Current guidelines vary, with the IDSA recommending three antibiotics for CRE infections and European guidelines prioritizing ceftazidime–avibactam and meropenem–vaborbactam.
While adverse events from novel antibiotics are generally mild to moderate, their long-term safety is still under review. Resistance to ceftazidime–avibactam and ceftolazone–tazobactam is an increasing concern. Antimicrobial sensitivity testing (AST) and identifying resistance mechanisms are critical for selecting appropriate therapies, particularly for patients at high risk of infections with resistant bacteria. Combination therapy with older antibiotics has not shown increased efficacy and may lead to higher toxicity. For CRAB, at least two active agents are recommended due to concerns over single-agent efficacy.
Source: Almyroudi MP, Chang A, Andrianopoulos I, Papathanakos G, Mehta R, Paramythiotou E, Koulenti D. Novel Antibiotics for Gram-Negative Nosocomial Pneumonia. Antibiotics (Basel). 2024 Jul 5;13(7):629. doi: 10.3390/antibiotics13070629. PMID: 39061311; PMCID: PMC11273951
You Might Also Like

Advances in the treatment of invasive fungal disease
Real-World Use of Isavuconazole as Primary Therapy for Invasive Fungal Infections in High-Risk Patients with Hematologic Malignancy or Stem Cell Transplant