Introduction
Triazole antifungals like voriconazole, posaconazole, and isavuconazole are used to treat invasive fungal infections like pulmonary aspergillosis. Triazoles inhibit cytochrome P450 enzymes (CYP450) and cause fungal cell death by blocking ergosterol synthesis. Many factors have been linked to variability in voriconazole and posaconazole exposure, including altered intestinal absorption and drug interactions. Therapeutic drug monitoring (TDM) is important to guide the treatment of voriconazole and posaconazole. For more than a decade, voriconazole has been considered the first-line treatment for invasive aspergillosis. When used as first-line treatment for invasive aspergillosis, posaconazole was recently found to be non-inferior to voriconazole, with participants in the posaconazole group experiencing fewer treatment-related adverse events than those in the voriconazole group. When compared to voriconazole in the same setting, isavuconazole also demonstrated non-inferior efficacy and a significantly better safety profile.
While the three triazoles have similar efficacy in patients with invasive aspergillosis, their effects on liver-mediated drug metabolism are significantly different. There is already evidence of a voriconazole-flucloxacillin interaction that results in subtherapeutic voriconazole plasma concentrations. In this case report, we describe a similar interaction between posaconazole and flucloxacillin.
Case Presentation
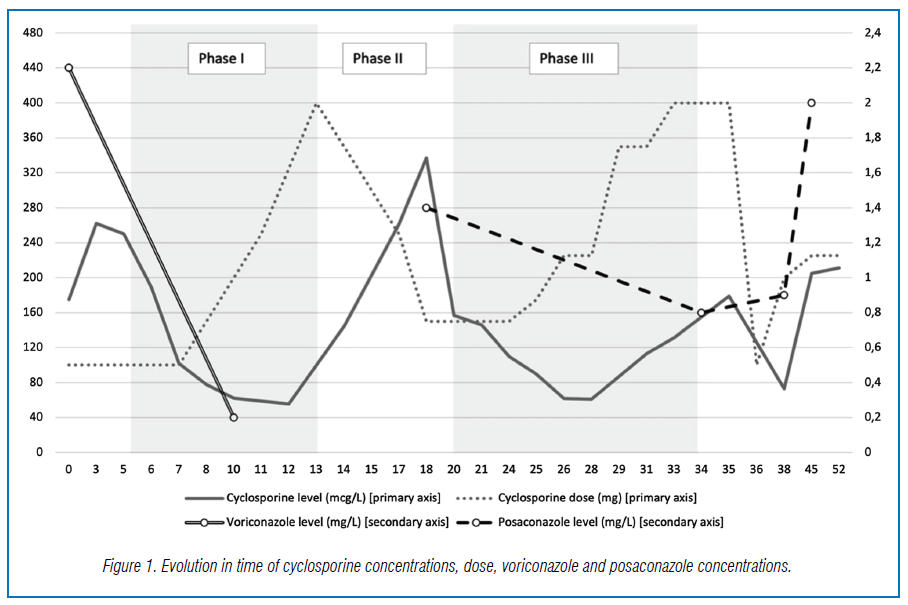
A 60-year-old male who had a double lung transplantation for end-stage chronic obstructive pulmonary disease was being treated with voriconazole for invasive pulmonary aspergillosis (IPA). During this treatment he presented at the emergency room and was diagnosed with endocarditis for which a combination of amoxicillin, flucloxacillin and gentamicin was initiated. A known interaction between voriconazole and flucloxacillin was observed, with a drop of the voriconazole levels, and treatment for IPA was switched to posaconazole. Interestingly an identical drop in concentrations of posaconazole was noted from 1.4 to 0.8 mg/L consistent with an interaction with flucloxacillin.
At the same time, cyclosporine concentrations also decreased, from 337 to 61 mcg/L. This is summarized in Fig. 1. After ending the treatment for endocarditis, the patient had a catheter infection for which flucloxacillin was reinitiated. Unexpectedly we saw a similar immediate drop in posaconazole levels, recovering after ending treatment with flucloxacillin.
Conclusions
We describe a new interaction between posaconazole and flucloxacillin. Presumably the underlying mechanism is activation of the pregnane X receptor by flucloxacillin, which can induce cytochrome P450, uridine glucuronosyl transferase (UGT1A4) and P-glycoprotein. We advise caution when combining flucloxacillin and triazoles, because interactions may lead to undertreatment of invasive aspergillosis.
Source: Verfaillie, S., Godinas, L., Spriet, I. et al. Interaction between posaconazole and flucloxacillin in a lung transplant patient: decrease in plasma exposure of posaconazole and possible undertreatment of invasive aspergillosis: case report. BMC Pulm Med 22, 110 (2022). https://doi.org/10.1186/s12890-022-01904-4