Introduction
The treatment of invasive fungal infections in liver transplant recipients is difficult because they are linked to increased morbidity and mortality. Despite a lack of clinical evidence, antifungal combination therapy is frequently thought to increase response rates in a patient population with compromised immune systems. In this article, we describe a case of refractory invasive candidiasis in a liver transplant patient that was successfully treated with isavuconazole and high-dose liposomal amphotericin B.
Among other tolerable side effects, the antimycotic combination treatment was able to cure a bloodstream infection with C. glabrata and resulted in the regression of bilomas. There have been no prior reports of the antifungal combination therapy mentioned above being used in liver transplant recipients. This is the first report describing the successful combination of isavuconazole (ISA) and liposomal amphotericin B (AMB) in a liver transplant recipient with refractory invasive candidiasis.
Case Report
A 52-year old female, who underwent LT past 3 months due to primary biliary cirrhosis, was admitted because of fever up to 40 °C. Endoscopic retrograde cholangiography (ERC) had demonstrated ischemic-type biliary lesions, characterized by intrahepatic bile duct strictures, in the absence of perfusion restrictions. Therapeutic ERC with double pigtail stent replacement was performed. With similar detection of both bacteria in the bile culture, a biliary focus seemed very likely.
During hospitalization the patient developed infection- associated progressive neutropenia (neutrophil nadir 0.74 G/l on day 4). Systemic candidiasis was diagnosed for the first time in the follow-up blood cultures on hospital day 8 based on the evidence of C. glabrata. Candida sepsis was diagnosed due to organ dysfunction with a Sequential Organ Failure Assessment (SOFA) score > 2 points. A biloma in liver segment VI/VII was detected for the first time on day 10 by abdominal sonography.
Laboratory findings consisted of slightly increasing transaminases (Fig. 1). An endophthalmitis was ruled out within a week after diagnosis. Extensive imaging, including echocardiography, orthopantomography and magnetic resonance imaging (MRI) of the spine did not reveal any evidence of an infection focus with C. glabrata.
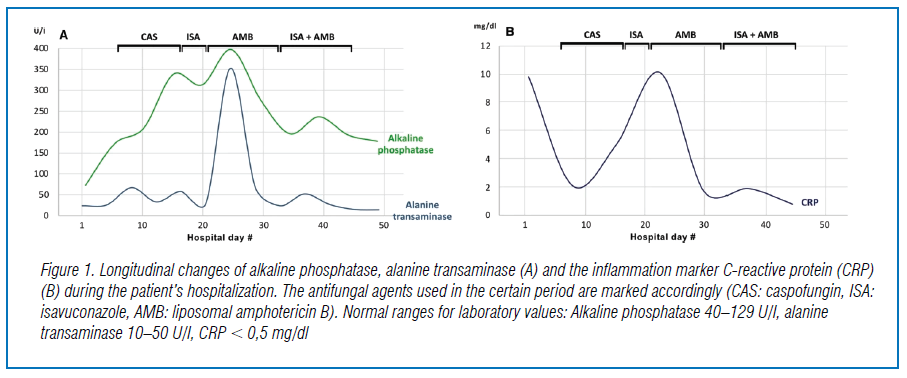
Due to persistent fungemia and recurrent episodes of fever, the intravenous antimycotic therapy was converted to isavuconazole (ISA; 200 mg three-times daily for two days, followed by 200 mg once daily). Shortly after switching to isavuconazole, both aspartate aminotransferase (AST) and alanine aminotransferase (ALT) decreased. However, further MRI imaging on hospital day 19 showed new bilomas with a maximum size of 23,8 × 15,2 mm (Fig. 2) In liver segments VII und VIII and an increasing expansion of bile ducts. Because of complicated structural conditions in the transplanted liver, stent replacement was not possible. Bile drainage was optimized by implantation of three new stents.
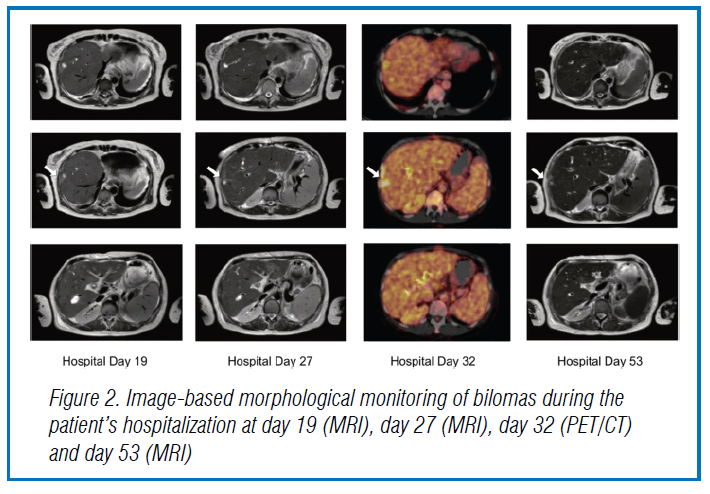
Increased metabolic activity of the known lesions in liver segment VIII were demonstrated by positron emission tomography-computed tomography (PET/CT), consistent with ascending cholangitis. Due to the complex anatomical conditions of the transplanted liver, further intervention by ERC was decided to be forgone. Subsequently we initiated an intensified dual antifungal therapy with high doses of liposomal amphotericin B (daily dose of 6 mg/kg of body weight) and isavuconazole (200 mg three-times daily for two days, followed by 200 mg once daily) on hospital day 34. The intravenous antifungal combination therapy was continued for 14 days after the first negative blood culture and stopped afterwards. Six days after completion of therapy, a follow-up MRI scan of the liver was performed, where cholangitis and bilomas showed to be regressed (Fig. 2).
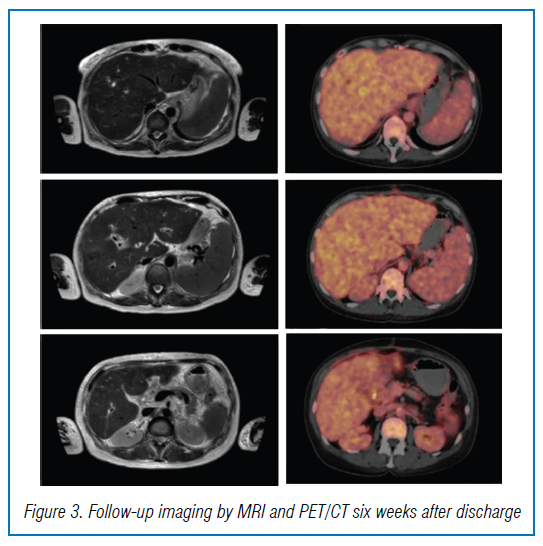
Ten days after discontinuation of dual antifungal therapy an antifungal prophylaxis was administered with posaconazole (300 mg twice on day 1, followed by 300 mg once a day for five weeks). Since this substance has been shown to provide high quality evidence in preventing IFI among immunocompromised patients. Follow-up imaging was performed six weeks after discharge and showed further regression of bilomas compared to the previous examination (Fig. 3). A PET/CT demonstrated lacking metabolic activity of the formerly hypermetabolic sites, consistent with a reduced inflammatory activity. Furthermore, there was no evidence of C. glabrata in the follow-up blood cultures. Of note, creatinine levels had decreased subsequently and were only slightly elevated at the follow-up visit.
Conclusion
For doctors, invasive fungal infections (IFI) in immunocompromised patients present a very difficult situation. This report explains that in a liver transplant recipient with invasive candidiasis, antifungal co-treatment with isavuconazole (ISA) and liposomal amphotericin B (AMB) offers efficacy and a favourable side effect profile. Thus, antimycotic combination therapy may be a promising treatment option for immunocompromised patients with persistent candidemia. To confirm the beneficial effects of dual antifungal therapy in this patient population, additional research is required.
Source: Source – Odysseos, G., Mayr, U., Bozsaki, G. et al. Isavuconazole and Liposomal Amphotericin B as Successful Combination Therapy of Refractory Invasive Candidiasis in a Liver Transplant Recipient: A Case Report and Literature Review. Mycopathologia 187, 113–120 (2022). https://doi.org/10.1007/s11046-021-00599-1