
Introduction
This article discusses community-acquired pneumonia (CAP), which accounts for approximately 2.2% of emergency department visits in the United States. Bacterial, viral, and fungal pathogens can cause infectious pneumonia, with Streptococcus pneumoniae and Haemophilus influenzae being the leading causes of bacterial pneumonia worldwide. Viral pneumonia is underdiagnosed but is becoming easier to detect with the availability of molecular diagnostic tests. One in 3 CAP cases are caused by a viral pathogen, with rhinoviruses, influenza viruses, and coronaviruses being the most common. Pneumonias caused by fungal pathogens are rare in immunocompetent individuals but pose a life-threatening risk to those with a compromised immune response. Emergency medicine providers must consider the possibility of fungal infection in at-risk patient populations to ensure early diagnosis and effective treatment. The article provides evaluation and treatment recommendations for CAP, based on established guidelines, but emphasizes caution in managing SARS-CoV-2 pneumonia due to the relative paucity of data and the frequency of iterations in guidelines and suggestions.
Community-Acquired Bacterial Pneumonia
Epidemiology and cause
Community-acquired pneumonia (CAP) affects over 5 million people in the US annually, with higher incidences in males and African Americans, and mortality rates higher in women. The causes of CAP can be typical or atypical organisms, including S pneumoniae, H influenzae, Staphylococcus aureus, Legionella, Mycoplasma pneumoniae, and Chlamydia pneumoniae. Bacterial and viral pathogens can coexist, making management challenging. Treatment of CAP is dependent on the cause of the infection, and categorization of the organism as typical or atypical. While S pneumoniae and K pneumoniae are the most common causes, Methicillin-resistant Staphylococcus aureus (MRSA) is the most common cause of health care–associated pneumonia. Ventilator-associated pneumonia has a high prevalence of multidrug-resistant bacteria. An increase in overall antimicrobial resistance by gram-negative bacteria has also been observed, increasing morbidity, mortality, and healthcare-associated costs.
Clinical presentation
Community-acquired pneumonia (CAP) has a varied clinical presentation and can be caused by different organisms, requiring specific diagnosis and treatment. Hallmark symptoms of bacterial pneumonia include cough, fever, chest pain, and confusion in the elderly. Atypical pathogens may cause extrapulmonary symptoms like gastrointestinal upset. Improved and rapid diagnostic testing has enabled better diagnosis and treatment of CAP in recent years.
Diagnosis/treatment
In 2019, the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS) established revised guidelines for the diagnosis and treatment of CAP. Criteria are outlined for determining severe CAP based on the following minor and major symptoms and diagnostic findings:
• Sputum cultures: Recommended only in patients meeting criteria for severe disease, especially if requiring mechanical ventilation. There is lack of evidence to support the use of sputum cultures in outpatient settings.
• Blood cultures: Recommended in patients meeting criteria for severe disease, those being treated empirically for MRSA or Pseudomonas aeruginosa, those with a history of MRSA or P aeruginosa, or those hospitalized within the past 90 days. These recommendations do have a low quality of evidence, although blood cultures continue to remain part of most institutional clinical pathways in the diagnosis of CAP. Given the overlap of CAP and sepsis, utilization of blood cultures is appropriate. Data prove that positive blood cultures within 10 hours of admission have shown an increased risk of mortality; however, only 40% of blood cultures drawn at initial presentation are positive.
• Molecular diagnostic testing/polymerase chain reaction testing: Recommended testing for influenza and SARS-CoV-2 based on local transmissibility data and prevalence. Molecular diagnostic tests have an overall 70% to 80% sensitivity rate and 99% to 100% specificity rate, therefore isolating cases of viral or atypical bacterial cause.
• Legionella and pneumococcal urinary antigen testing (UAT): Recommended only in the patient with severe CAP or in cases of high epidemiologic concern/recent travel (Legionella).
• Imaging: Chest computed tomography (CT) is considered the gold standard in detection of both CAP and viral pneumonia; however, cost, accessibility, and radiation continue to be limiting factors. Chest radiograph alone has a sensitivity of 38% to 76%; however, when combined with molecular testing, sensitivity and specificity increase. Ultrasonography has been shown to have sensitivity rates of 80% to 90% in the detection of pneumonia. The IDSA/ATS guidelines no longer recommend routine use of chest radiograph in follow-up after a pneumonia diagnosis.
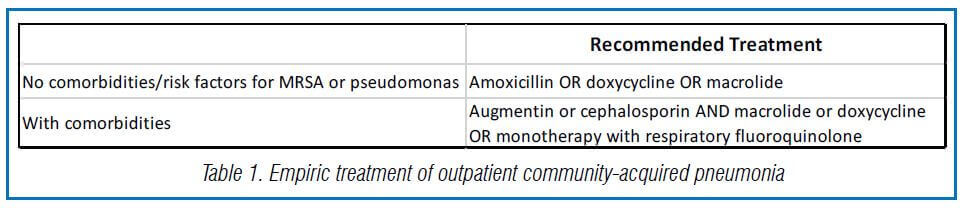
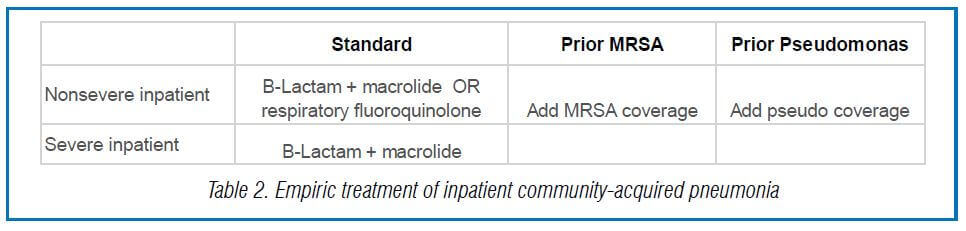
Treatment decisions vary greatly owing to differences in risk assessment outcomes indicated, comorbidities, and likelihood of MRSA infection. Tables 1 and 2 outline the recommended outpatient and in-hospital initial treatments for CAP.3.
Prognosis
Outcomes of treatment largely depend upon age of onset, hospitalization status with treatment, and the presence of comorbidities. The overall mortality for pneumonia may be up to 30% if left untreated. Overall prognosis, however, is tremendous in a healthy patient. Most individuals respond to treatment within 48 to 72 hours of initial management, both in hospital and at home. Respiratory failure, sepsis, organ failure, coagulopathy, and exacerbation of comorbidities are complications to consider as a result of CAP.
Community-Acquired Viral Pneumonia
Epidemiology
The article discusses viral pneumonia, mainly focusing on COVID-19 caused by the SARS-CoV-2 virus. As of publication, there have been over 470 million confirmed cases of COVID-19 globally, with 6 million deaths reported to WHO and CDC. Ten vaccines have been granted an emergency use listing by WHO, and vaccination rates vary by country. Before the COVID-19 pandemic, other viruses caused pneumonia, but COVID-19 has contributed to the majority of viral pneumonia cases. Vaccination has been proven effective in decreasing mortality and hospitalization rates for COVID-19 infections, including against the delta and omicron variants.
Clinical presentation
This passage discusses the pathology, transmission, symptoms, and diagnosis of COVID-19 pneumonia. COVID-19 pneumonia is highly virulent and transmissible through respiratory particles, and both symptomatic and asymptomatic individuals can spread the virus. Symptoms range from mild to severe, with older individuals and those with comorbidities at higher risk for severe illness. Diagnostic testing includes laboratory markers such as procalcitonin and inflammatory markers, as well as chest imaging. CT imaging is more sensitive than chest radiography for early detection and monitoring disease progression.
Treatment
The American Academy College of Emergency Physicians recommends the following specific approach based on severity :
• Mild to moderate signs of COVID-19: These patients may benefit from nonpharmacologic treatment alone. These options include home oxygen therapy, breathing exercises, continual ambulation, adequate sleep, and a consistent healthy diet with adequate hydration.
• Severe signs of COVID-19: Recommendations for oxygen support using a nasal cannula with titration to 6 L, high-flow nasal cannula (HFNC) or high-velocity therapy, noninvasive positive pressure ventilation if HFNC is not available, or a consideration of prone positioning if patient can be monitored closely. Proning of patients is contraindicated in the presence of respiratory distress.
• Endotracheal intubation is considered: If a goal of oxygenation at 92% to 96% cannot be maintained, low-tidal volume, plateau pressures less than 30 cm, higher positive end-expiratory pressure, or if a patient experiences refractory hypoxemia with prone ventilation. Currently, sufficient data do not exist to determine the benefit of extracorporeal membrane oxygenation in the management of severe COVID-19 pneumonia. Recommendations for pharmacologic management of COVID-19 are not made specific to those patients with or without pneumonia. Recommendations are based on outpatient or inpatient management and therefore on disease severity. Current recommendations are summarized as follows:
• Remdesivir is the only antiviral medication approved by the Food and Drug Administration (FDA) for the treatment of COVID-19.
• Ritonavir-boosted nirmatrelvir (Paxlovid) and SARS-CoV-2 monoclonal antibodies have been given an Emergency Use Authorization from the FDA.
• Nonhospitalized patients: All patients with confirmed SARS-CoV-2 who are at risk for progressing to severe disease should receive (in order of preference): paxlovid, sotrovid, remdesivir, and molnupiravir. Systemic corticosteroids are not recommended.
• Hospitalized patients: Remdesivir is recommended in all patients requiring admission for SARS-CoV-2. In addition, dexamethasone is recommended if supplemental oxygen is required. Finally, and dependent on severity of disease and progression, tocilizumab is recommended.
• The National Institutes of Health and CDC update detailed guidelines regularly, including the use of heparin.
Prognosis
The prognosis of COVID-19 pneumonia varies widely and is influenced by individual comorbidities, patient demographics, and hospital staffing. Mortality is highest among patients with ARDS, with a wide range of reported mortality rates from 12% to 78%. Death from COVID-19 can result from complications such as arrhythmias, cardiac arrest, or pulmonary embolism. Rapid symptom progression does not necessarily contribute to worsened outcomes.
Community-Acquired Fungal Pneumonia
Cause/epidemiology
Fungal pneumonia can affect neutropenic and nonneutropenic patients, and risk factors include chemotherapy, stem cell transplant, prolonged steroid use, AIDS/HIV infection, chronic obstructive pulmonary disease, diabetes, liver or renal failure, severe immunodeficiency, and ICU patients. Common fungal pathogens causing pneumonia include coccidioidomycosis, Histoplasma capsulatum, Aspergillus fumigatus, Candida albicans, Cryptococcus neoformans, blastomyces, and Pneumocystis jiroveci.
Clinical presentation
Patients with fungal pneumonia, whether neutropenic or nonneutropenic, can present with a range of symptoms, including cough, fever, dyspnea, increased sputum production, or pleuritic chest pain. In nonneutropenic patients, symptoms may be asymptomatic until later stages of the disease. Generalized symptoms such as lightheadedness, malaise, weakness, headache, nausea/vomiting, joint pain, and rash can also be associated with fungal pneumonia. It is important to rule out other disease processes with appropriate history, physical examination, and laboratory and diagnostic imaging.
Treatment
Treatment of fungal infection is often targeted and based on blood and/or sputum culture results:
• Aspergillosis: Initial therapy with voriconazole is recommended for most patients. The preferred alternative for patients that cannot tolerate the recommended initial therapy is a combination of posaconazole and isavuconazole.
• P jiroveci: Initial therapy with trimethoprim/sulfamethoxazole is recommended.
• H capsulatum: If less than 4 weeks of an acute lung infection, no treatment is recommended. If greater than 4 weeks of an acute lung infection, a 3-month course of itraconazole is recommended.
Discussion
The article discusses the importance of emergency medicine providers being able to identify and manage patients with pneumonia, including the recent increase in hospital admissions due to COVID-19-associated pneumonia. Guidelines for the management of bacterial, viral, and fungal pneumonias are established collaboratively by organizations such as IDSA, CDC, and ATS and are regularly updated. Demographic and seasonal factors and individual patient risk factors must also be considered when guiding treatment.
Source: Dillon K, Garnick B, Fortier M, Felicia B, Fulton A, Dumont C, Dorval B, Gardella K. The Management of Infectious Pulmonary Processes in the Emergency Department: Pneumonia. Physician Assist Clin. 2023 Jan;8(1):123-137. doi: 10.1016/j.cpha.2022.08.005. Epub 2022 Nov 24. PMID: 36448036; PMCID: PMC9688359.


