
Introduction
Candida glabrata is a new Candida species that causes infections ranging from minor to life-threatening systemic illness. Echinocandins and azoles are commonly employed as first-line therapy to treat C. glabrata infections, however there is a growing prevalence of resistance to these antifungal drugs in patients. C. glabrata is the second most prevalent species discovered in women with vulvovaginal candidiasis (VVC) after C. albicans, with a frequency ranging from 3.4 to 20% across America, Europe, and Australia. C. glabrata exhibits greater rates of azole antifungal resistance than other Candida species, including C. albicans, C. tropicalis, and C. parapsilosis.
The increasing resistance to azoles and echinocandins, as well as the toxicity and lack of oral bioavailability of amphotericin B, necessitates the development of novel antifungals. Ibrexafungerp is a first-in-class glucan synthase inhibitor with oral availability that was created to combat antifungal resistance. Ibrexafungerp has extensive in vitro activity against C. glabrata species and has also been demonstrated to be effective in low pH settings, implying its efficacy in treating vulvovaginitis.
Mechanism of Action of Ibrexafungerp
The goal of the development of ibrexafungerp is to be the first oral and IV GSI that may be used in the treatment and prevention of diverse fungal infections, including life-threatening illnesses as well as superficial infections (e.g., vulvovaginal candidiasis). Ibrexafungerp and echinocandins both inhibit -1, 3-D-glucan synthase; however, their structures differ and they interact with the target enzyme differently, resulting in a reduced rate of resistance to ibrexafungerp. Furthermore, the binding site for both appears to be different.
In Vitro and In Vivo Activity
Ibrexafungerp displayed potent in vitro activity against a wide range of Aspergillus species and Candida isolates, including isolates resistant to azoles and echinocandins. Additionally, ibrexafungerp has uniform and potent activity against C. auris, an emerging multidrug-resistant fungus, which was demonstrated in several studies. Interestingly, studies showed that ibrexafungerp inhibited cell growth and division of C. auris.
These data suggest that in addition to the glucan synthase inhibition effect, this drug may have a separate target or may affect this enzyme through different mechanisms. Ibrexafungerp has fungicidal activity against Candida species which was demonstrated in a time-kill study in which ibrexafungerp showed activity comparable to that of caspofungin. It also showed potent in vitro activity against Candida species in a low pH environment suggesting a therapeutic advantage of ibrexafungerp in the treatment of vaginal Candida infections.
Pharmacokinetics
In vitro bioavailability was assessed using Caco-2 cell monolayers as a predictor of absorption across the gut. The mean apparent permeability was 8.9 ± 0.78 × 10− 6 cm/s for 5 µM ibrexafungerp indicating a good oral absorption. It also demonstrated high protein binding (99.5–99.8%) in different species, which is expected for a compound with a lipophilic nature.Ibrexafungerp achieved maximum plasma concentrations (Cmax) between 4 and 6 h reflecting a prolonged absorption phase after oral administration.
Furthermore, assessment of the distribution of ibrexafungerp between plasma and kidney tissue displayed a tissue concentration 20- to 25-fold greater than that seen in plasma, indicating high tissue penetration. Common adverse events (AE) observed were mostly in the form of diarrhea, abdominal pain, nausea, vomiting, and flatulence.
Ibrexafungerp and Candida glabrata
A compilation across five independent studies was performed to identify the in vitro MIC data for ibrexafungerp against C. glabrata isolates with fks mutations (30 fks1 and 49 fks2). Ibrexafungerp showed activity against 78% of C. glabrata isolates with fks mutations. Additionally, ibrexafungerp demonstrated greater in vitro activity compared to micafungin and caspofungin against fks mutated C. glabrata strains. The MIC50 of ibrexafungerp against fks mutant C. glabrata ranged from 0.5 to 1 µg/ml, MIC50 of caspofungin ranged from 0.5 to 4 µg/ml, and micafungin ranged from 0.125 to 0.25 µg/ml
In Vitro Activity at Different pH Levels
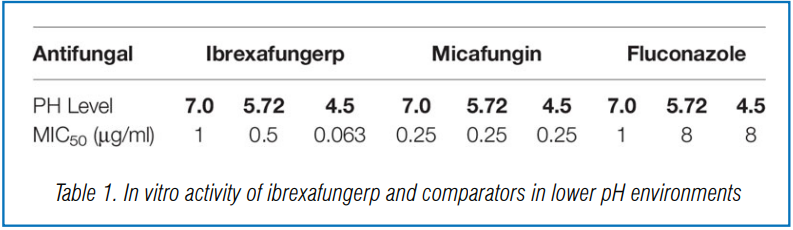
Larkin et al. demonstrated the efficacy of ibrexafungerp in lower pH environments by evaluating the activity of the drug against Candida species isolated from patients with vulvovaginitis. The in vitro activity of ibrexafungerp was shown to be enhanced in lower pH environments. Against ten C. glabrata isolates, the MIC50 values of ibrexafungerp tested at pH levels of 7.0, 5.72, and 4.5 were 1, 0.5, and 0.063 µg/ml, respectively. In comparison, the MIC50 value of micafungin remained the same regardless of pH (0.25 µg/ml), while the MIC50 values of fluconazole at pH levels of 7.0, 5.72, and 4.5 were 1, 8, and 8 µg/ml, respectively (Table 1).
Effect Against Biofilms
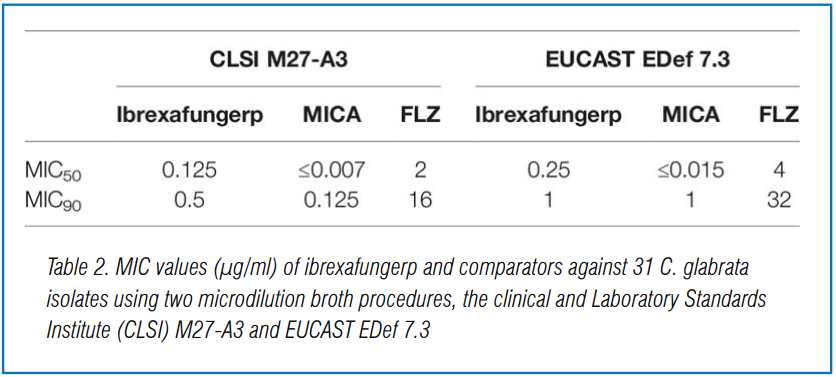
In a study performed in Madrid, Spain, the antifungal activity of ibrexafungerp, micafungin, and fluconazole as evaluated against planktonic and sessile Candida albicans and non-albicans; including 31 C. glabrata. Antifungal susceptibility testing was performed using the Clinical and Laboratory Standards Institute (CLSI) M27-A3 and EUCAST EDef 7.3 microdilution broth procedures.
The MIC50 and MIC90 values (defined as the concentration that inhibit 50% and 90% of isolates tested, respectively) of ibrexafungerp compared to untreated control were 0.125 and 0.25 µg/ml, and 0.5 and 1 µg/ml for CLSI and EUCAST, respectively. In contrast, the MIC50 and MIC90 of fluconazole were 2 and 4 µg/ml, and 16 and 32 µg/ml CLSI and EUCAST, respectively, while the MIC50 and MIC90 of micafungin were ≤0.007 and ≤0.015 µg/ml, and 0.125 and 1 µ g/ml CLSI and EUCAST, respectively (Table 2).
Activity of Ibrexafungerp In Vivo
Another study assessed ibrexafungerp activity against invasive candidiasis caused by C. glabrata. Four C. glabrata isolates were tested against four oral doses, 3.125, 12.5, 50, and 200 mg/kg of ibrexafungerp salt. Ibrexafungerp demonstrated potent activity in vivo against each isolate with a stasis endpoint achieved at a mean dose of 58.4 mg/kg. MIC range varied 8-fold (range, 0.03 to 0.25 µg/ml) achieving a mean tAUC/MIC of 315, and an fAUC/MIC of 0.63.
The maximum concentration of drug in serum increased from 0.04 µg/ml to 2.66 µg/ml over the dose range. Clinical Efficacy of Ibrexafungerp Another phase 3 open-label, single-arm study showed that oral ibrexafungerp provides favorable therapeutic response when used to treat refractory or intolerant Candida infections, namely C. glabrata. Of the 17 patients with invasive candidiasis/candidemia caused by C. glabrata, nine showed complete or partial response (52.9%), five had stable disease (29.4%), and three had their disease progress further (17.7%). Ibrexafungerp was also well-tolerated in patients with the most common adverse effect being gastrointestinal.
Summary and Conclusions
C. glabrata is a developing issue for mucosal and systemic bloodstream infections, and it is especially concerning due to its multidrug resistance to both azoles and echinocandins. Novel antifungal medicines in development, such as ibrexafungerp, a first-in-class triterpenoid antifungal, will provide therapy alternatives for these issues. Unlike previous echinocandins, ibrexafungerp can be administered orally, and it is generally safe and well tolerated, with gastrointestinal side effects being the most commonly reported. Several investigations have indicated that echinocandin antifungal medications, such as caspofungin and micafungin, have equivalent or superior in vitro activity against both wild-type and echinocandin-resistant C. glabrata isolates. However, more preclinical and clinical trials are needed to demonstrate the efficacy and safety of ibrexafungerp in treating fungal infections caused by C. glabrata and other types of invasive fungal illnesses.
Source: Gamal Ahmed, Chu Sherman, McCormick Thomas S., Borroto-Esoda Katyna, Angulo David, Ghannoum Mahmoud A. Front. Cell. Infect. Microbiol., 11 March 2021 | https://doi.org/10.3389/fcimb.2021.642358


