Aim
To evaluate the pharmacokinetics of colistimethate sodium and colistin in critically ill patients and correlate with clinical efficacy and renal function.
Materials and Methods
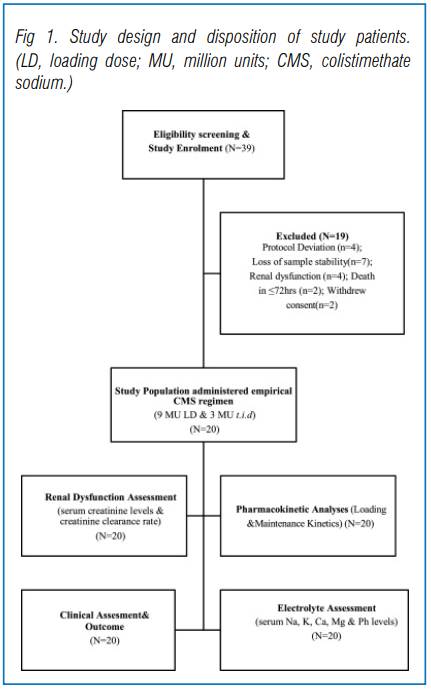
This prospective observational study was conducted from 01 February to 01 October 2017 at a large academic tertiary care hospital in India. Critically ill adult patients from Intensive Care Unit (ICU) and non-ICU locations, with normal renal function (creatinine clearance ≥80 mL/min) requiring at least 5 days of intravenous colistin for treatment of MDR Gram-negative infections were included. Detailed demographic, clinical, laboratory and microbiology data on each study patient were recorded (Fig 1). Concentrations of CMS and formed (free) colistin A and colistin B in plasma were determined using a validated HPLC-MS/MS method. CMS concentration was obtained after deducting formed colistin concentration from total colistin at each time point. Serum creatinine measured at enrollment was considered the baseline value. Serum creatinine was measured daily until end of therapy and assessment of nephrotoxicity was performed using the RIFLE criteria.
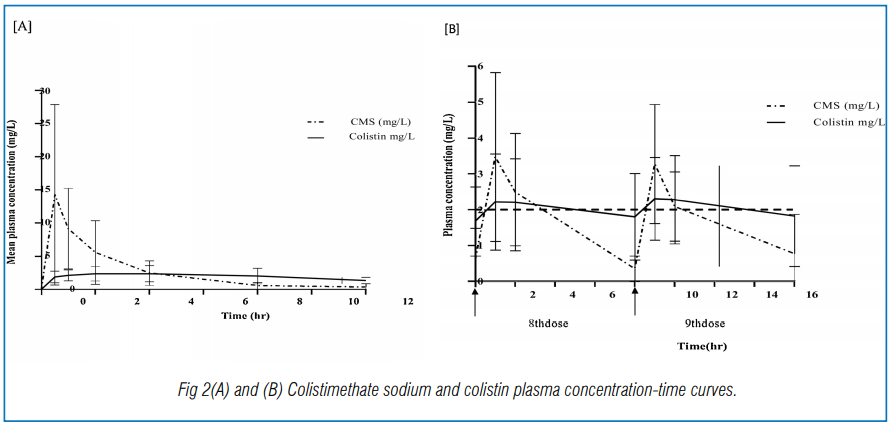
Twenty critically ill adult patients with colistin-susceptible multidrug-resistant (MDR) infections and normal renal function were treated with intravenous colistimethate sodium. 9 million units (270 mg CBA) loading dose was followed by maintenance (MD) of 3 million units t.i.d. 24 hours later patients were evaluated for clinical cure (CC) at the end of therapy. Patient characteristics and plasma colistin levels at 0, 0.5, 1, 2, 4, 8 and 12 hours after the loading dose and at 1, 2 and 8 hours after the eighth and ninth infusion of MD were evaluated.
Colistimethate sodium and colistin levels were measured by high-performance liquid chromatography and tandem mass spectrometry (HPLC-MS/MS) (Fig 2 (A) & (B).
Results
Among the patients with pneumonia, all of the seven patients with Klebsiella pneumoniae were sensitive to colistin (MICs ≤0.5–1 µg/mL) and the majority (6/7) were carbapenem resistant. A combination therapy of colistin and meropenem showed clinical response in three (43%) cases. This combination therapy was also administered in four of the five Acinetobacter spp. pneumonia cases, while one received a combination of colistin and tigecycline. All the Acinetobacter spp. isolates were carbapenem resistant. Colistin sensitivity ranged from MIC ≤ 0.5 to 1 µg/mL. Clinical cure was 50% (10/20). Mean peak loading dose concentrations were 3 ± 1.1 mg/L (1.75–5.14) and 2.37 ± 1.2 mg/L (1.52–5.54) for ‘cure’ and ‘failure’ groups, respectively (p = 0.13).
Mean steady-state (Cssavg) concentrations were 2.25 ± 1.3 mg/L and 1.78 ± 1.1 mg/L in ‘cure’ and ‘failure’ groups, respectively (p = 0.19). Nephrotoxicity was 5% on day 7 of therapy. However, bacteriological cure could not be correlated with PK/PD.
Conclusion
Subtherapeutic Cssavg with clinical failure and lower efficacy without significant nephrotoxicity highlights the need for therapeutic drug monitoring to guide colistin dosing.
Source: International Journal of Infectious Diseases, VOLUME 100, P497-506, https://doi.org/10.1016/j.ijid.2020.08.010